Part One of Depressive Disorders covers specifiers. Specifiers are used to further define the characteristics that accompany a mental health diagnosis. These specifiers are important because diagnosis determines the course of treatment. The following specifiers are defined below: anxious distress, mixed features, melancholic features, atypical features, psychotic features, mood-congruent psychotic features, mood-incongruent psychotic features, catatonia, peripartum onset, and seasonal pattern. Some of these specifiers may sound familiar to you because they are also used when specifying Bipolar and Related Disorders.
Specifiers for Depressive Disorders
Mixed Features
There are four criterion for the “with mixed features” specifier. Criterion A states that the individual must experience three or more symptoms of mania or hypomania almost every day during most of the depressive episode. A detailed description of mania and hypomania can be found in the Part Two of Bipolar and Related Disorders.
Criterion B requires that the symptoms of depression, mania and/or hypomania are a change from the person’s typical behavior and that the changes are observable by others. Criterion C is specifically for individuals whose symptoms meet full criteria for either mania or hypomania. In these cases, the individual’s diagnosis should be either Bipolar I or Bipolar II Disorder. Criterion D states that the “symptoms are not attributable to the physiological effects of a substance” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Catatonia
Catatonia or catatonic behavior is a noticeable decrease in the level and intensity of which an individual interacts with or responds to their environment. The catatonia specifier is applied to Depressive Disorders diagnosis when catatonic features are present during the majority of the individual’s depressive episode. Details about catatonia can be found in Part Three of Schizophrenia Spectrum and Other Psychotic Disorders.
Melancholia Features
This specifier is applied when its features are present at the most severe stage of the individual’s depressive episode. There are two criteria for meeting the melancholia features specifier. Criterion A requires that the individual experience either loss of pleasure in the majority of their activities or a “lack of reactivity to usually pleasurable stimuli” (Diagnostic and Statistical Manual of Mental Disorders, 2013). Criterion B requires that the individual experience three or more of the following features:
- “A distinct quality of depressed mood or so-called empty mood
- Depression that is regularly worse in the morning
- Early-morning awakening (i.e., at least 2 hours before usual awakening)
- [Noticeable] psychomotor agitation or [delay]
- Significant anorexia or weight loss
- Excessive or inappropriate guilt”
(Diagnostic and Statistical Manual of Mental Disorders, 2013).
Psychotic Features
The psychotic features specifier is added to a diagnosis when the individual experiences delusions and hallucinations during a depressive episode. Delusions are beliefs that remain even when there is evidence that is contrary. Hallucinations occur when an individual involuntarily perceives an experience without any external stimuli. Details regarding delusions and hallucinations are described in the Introduction to Schizophrenia Spectrum and Other Psychotic Disorders.
Seasonal Pattern
The seasonal pattern specifier is used for individuals with recurrent major depressive episodes. The seasonal pattern specifier is added to a diagnosis when the depressive episode occurs during the same time of year and subsides during another time of year. The DSM-5 outlines four criteria that qualify symptoms for the seasonal pattern specifier.
One, the relationship between the change of the season and the change in mood from euthymic (‘normal’ mood) to a depressive mood or the reverse occurs regularly and during the same time of year. Two, the individual goes into full remission with the change of the season or at a particular time of year. An example of this is when depression lifts in the spring. Three, the individual’s mood episodes do not have non-seasonal changes. Four, seasonal mood episodes significantly outnumber any non-seasonal mood episodes during the individual’s lifetime.
Peripartum Onset
The peripartum onset specifier is reserved for describing the symptoms of depression that began during pregnancy or within four weeks of delivery (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Mood-Congruent Psychotic Features
This specifier is applied when the individual experiences delusions and hallucinations. It is important to note that these psychotic features must align with the “typical depressive themes of personal inadequacy, guilt, disease, death, nihilism [rejection of religious principles], or deserved punishment (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Mood-Incongruent Psychotic Features
The “mood-incongruent psychotic features” specifier is used when the “content of the delusions or hallucinations [that the individual experiences] does not involve typical depressive themes” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Specifiers for Major Depressive Disorder and Persistent Depressive Disorder
The following specifiers are only used for either Major Depressive or Persistent Depressive Disorder.
Anxious Distress
The anxious distress specifier is added to a diagnosis if the individual experiences two or more ‘anxious’ features during a major depressive episode or when also experiencing the symptoms of persistent depressive disorder. The number of symptoms experienced determines the severity of the distress. Experiencing two symptoms is considered mild; three symptoms is moderate; four or five symptoms is moderate to severe; and, experiencing four to five symptoms with motor agitation (involuntary and meaningless movement) is classified as severe. The Fifth Edition of the Diagnostic and Statistical Manual (DSM-5) outlines anxious features as follows: tension, restlessness, worry that makes concentration difficult, fear something horrible will occur, and feeling as though they may lose control.
Atypical Features
The atypical features specifier is added to a diagnosis when the following features are prevalent during a major depressive episode or when also experiencing the symptoms of persistent depressive disorder. The first necessary feature is mood reactivity which describes how an individual’s “mood brightens in response to actual or potential positive events” (Diagnostic and Statistical Manual of Mental Disorders, 2013). Secondly, the individual experiences two or more of the following features: “significant weight gain or increase in appetite; hypersomnia; leaden paralysis, [or a heavy feeling in the limbs]; and a long-standing pattern of [sensitivity to] interpersonal rejection that results in significant social or occupational impairment” (Diagnostic and Statistical Manual of Mental Disorders, 2013). Finally, the individual must not meet the criteria for the “with melancholic features” or “with catatonia” specifiers, which are described above, during the same depressive episode.
Stay Tuned for Part Two which differentiates Major Depressive Disorder and Persistent Depressive Disorder!
References
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA, American Psychiatric Association, 2013. Web. [access date: 2 May 2018]. dsm.psychiatryonline.org

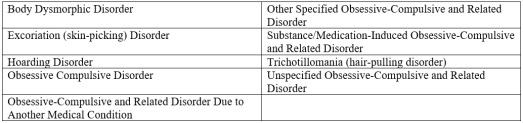 Each of these disorders has at least one common criterion: “the disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Each of these disorders has at least one common criterion: “the disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
