
What classifies a disorder as a form of Schizophrenia or another Psychotic Disorder?
Schizophrenia and psychosis are more complicated than a person simply hearing voices. The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders lists five domains that characterize Schizophrenia Spectrum and Other Psychotic Disorders. They are as follows: “delusions; hallucinations; disorganized thinking [and/or speech]; grossly disorganized or abnormal motor behavior, including catatonia; and negative symptoms” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Descriptions of Important Terms
Prior to describing the diagnostic criteria for the Schizophrenia Spectrum and Other Psychotic Disorders, the DSM-5 defines the five domains that characterize the disorders.
Delusions are beliefs that remain even when evidence that is contrary to the belief is presented. Delusions have many themes, the most common of which are persecutory and referential, which are defined below.
- “Persecutory Delusions: belief that one is going to be harmed, harassed, and so forth by an individual, an organization, or another group;
- Referential Delusions: belief that certain gestures, comments, environmental cues, and so forth are directed at oneself;
- Grandiose Delusions: when an individual believes that he or she has exceptional abilities, wealth, or fame;
- Erotomanic Delusions: when an individual believes falsely that another person is in love with him or her, [which is the root of stalking];
- Nihilistic Delusions: the conviction that a major catastrophe will occur; and,
- Somatic Delusions: preoccupations regarding health and organ function” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
In addition to these themes, delusions can also be considered bizarre. A delusion is classified as bizarre if it is highly improbable and if another individual from the same culture as the person experiencing the delusion does not understand it. There is an emphasis on culture because some cultures have widely held beliefs that are much different than beliefs that are held by the majority culture.
The DSM-5 (2013) gives the following examples to differentiate between bizarre and non bizarre delusions, “the belief that an outside force has removed his or her internal organs and replaced them with someone else’s organs without leaving any wounds or scars. An example of a nonbizarre delusion is the belief that one is under surveillance by the police, [the FBI, and the CIA], despite a lack of convincing evidence.”
Hallucinations occur when an individual involuntarily perceives an experience without any external stimuli. These clear and intense perceptions can be sensory, auditory, or visual. Auditory hallucinations are not the individual’s thoughts, but are instead a distinct voice that is either familiar or unfamiliar to the person.
Mild forms of hallucinations occur as part of our sleep cycle. Hallucinations that occur when falling asleep are called hypnagogic, and hallucinations that occur when waking up are referred to as hypnopompic. Although we typically do not remember these hallucinations, both of these are considered normal. It is important to note that hallucinations that are a result of psychosis occur while an individual’s mind is clear and when they are fully awake.
Disorganized Thinking is determined by listening to the individual’s speech. An individual’s thinking is considered disorganized when their speech inhibits their ability to effectively communicate. The DSM-5 (2013) describes three speech patterns that demonstrate disorganized thinking:
- “Derailment or Loose Associations: switching from one topic to another [while talking];
- Tangentiality: giving answers to questions that may be obliquely related or completely unrelated [and confuse the listener]; and,
- Incoherence or ‘Word Salad’: speech that is so severely disorganized that it is nearly incomprehensible”.
Grossly Disorganized or Abnormal Motor Behavior includes a wide range of movements and/or behaviors such as extremely rigid limbs, exceptionally flexible limbs, and holding a blank stare. These behaviors are typically identified when the individual is attempting to complete a specific task, especially one for daily living.
Catatonia or catatonic behavior is “a marked decrease in reactivity to the environment” (Diagnostic and Statistical Manual of Mental Disorders, 2013). The DSM-5 (2013) describes four types of catatonic behaviors:
- negativism, or resistance to instructions;
- maintaining a rigid, inappropriate or bizarre posture;
- mutism and stupor, which is a complete lack of verbal and motor responses; and,
- catatonic excitement, or purposeless and excessive motor activity without obvious cause.”
Other examples of catatonic behavior include, but are not limited to, “repeated stereotyped movements, staring, grimacing, and the echoing of speech” (Diagnostic and Statistical Manual of Mental Disorders, 2013). An individual does not have to be on the Schizophrenia Spectrum nor do they have to be diagnosed with a psychotic disorder to experience catatonia. Catatonic behaviors are also seen in depressive disorders.
Negative Symptoms are symptoms that decrease an individual’s ability to function normally. Negative symptoms include, but are not limited to, alogia, anhedonia, asociality, avolition, and diminished emotional expression. The two most prominent negative symptoms seen in schizophrenia spectrum and psychotic disorders are diminished emotional expression and avolition. The DSM-5 (2013) describes these symptoms as follows:
- “Alogia: diminished speech output;
- Anhedonia: the decreased ability to experience pleasure from positive stimuli or a degradation in the recollection of pleasure previously experienced;
- Asociality: the apparent lack of interest in social interactions;
- Avolition: a decrease in motivated self-initiated purposeful activities; and,
- Diminished Emotional Expression: reductions in the expression of emotions in the face, eye contact, intonation of speech, and movements of the hand, head, and face that normally give an emotional emphasis to speech”.
Names of the Disorders within the Class
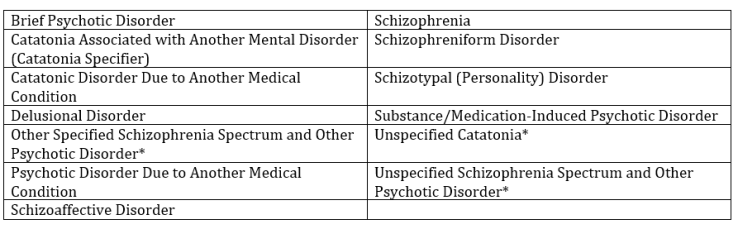
*We will not cover the unspecified or other specified disorders in this blog.
Each of these disorders has at least one common criterion: “the disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning” (Diagnostic and Statistical Manual of Mental Disorders, 2013). This requirement is typically listed as the last diagnostic criteria for each of the disorders within the class.
Organization of this Blog Series
The Schizophrenia Spectrum and Other Psychotic Disorders blog will have three parts: Part One will cover Schizoaffective Disorder; Schizophrenia; Schizophreniform Disorder; and Schizotypal (Personality) Disorder. Part Two will cover Brief Psychotic Disorder; Psychotic Disorder Due to Another Medical Condition; and Substance/Medication-Induced Psychotic Disorder. Finally, Part Three of Schizophrenia Spectrum and Other Psychotic Disorders will cover Catatonia Associated With Another Mental Disorder (Catatonia Specifier); Catatonic Disorder Due to Another Medical Condition; and Delusional Disorder.
Click HERE to read the introduction to this blog series, Mental Health Diagnoses!, which covers how diagnosis using the Diagnostic and Statistical Manual- 5 (DSM-5) works.
Stay Tuned for Part One!
References
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA, American Psychiatric Association, 2013. Web. [access date: 20 January 2018]. dsm.psychiatryonline.org

4 Replies to “Introduction to Schizophrenia Spectrum and Other Psychotic Disorders!”