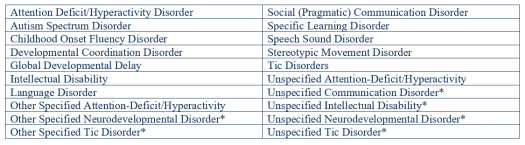
Part Three of Neurodevelopmental Disorders will cover disorders of movement. These include Developmental Coordination Disorder, Stereotypic Movement Disorder, and Tic Disorders, all of which are discussed below.
Click HERE if you would like to review the blog that introduces this series on Mental Health Diagnoses!
Developmental Coordination Disorder
Clumsy, awkward, and ‘all thumbs’ are typically how people describe someone who lacks coordination. While we have all experienced moments of disharmony, for some, lack of coordination hinders daily functioning. In these cases, it is necessary to consider whether or not the individual has Developmental Coordination Disorder.
Developmental Coordination Disorder is characterized by the impairment of motor coordination. This can be ‘tripping over your own feet’, trouble standing on one foot, difficulty using scissors, and/or problems tying shoelaces. Developmental Coordination Disorder also includes slow and inaccurate motor skill functioning (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Criteria for Diagnosis
Diagnosis requires a detailed developmental and medical history, a physical examination, and assessments of the individual while they are in multiple contexts, such as work or school. Multiple assessments and a detailed history are needed because an individual may meet motor milestones such as crawling and walking, but they may also be “delayed in developing skills such as negotiating stairs, pedaling, or buttoning shirts” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
The individual’s motor skill impairment must significantly interfere with their daily activities: getting dressed, using tools, and participating in group physical activities. Developmental Coordination Disorder can manifest in either gross or fine motor skills.
Stereotypic Movement Disorder
There have been several memes, gifs, and short videos circulating throughout social media with the caption “always on beat”. The clips usually show a celebrity rocking back and forth as though they were in sync with music playing in the background. It is possible that the individuals shown in these clips are simply rocking to the beat of a song that is stuck in their head and not that they are unable to control their movements. The inability to control repetitive movements, such as rocking side to side, is one of the characteristics that describe Stereotypic Movement Disorder.
Stereotypic Movement Disorder is “repetitive, seemingly driven, and apparently purposeless motor behavior” (Diagnostic and Statistical Manual of Mental Disorders, 2013). While there are many examples of stereotypic movements, individuals with this diagnosis typically have unique or “signature” movements. Some of these movements are classified as ‘with self-injurious behavior’ or ‘without self-injurious behavior’. Movements such as eye poking, biting, and slapping are examples that would require an individual be given the ‘with self-injurious’ specifier, and movements such as flapping the arms, rotating feet and hands, head nodding, and body rocking are specified as ‘without self-injurious behavior’ (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Criteria for Diagnosis
Diagnosis with Stereotypic Movement Disorder requires the individual to have repetitive, purposeless movements that interfere with their social, occupational, or academic lives, and/or may cause injury; its onset must begin in the early developmental period; and, the repetitive movements must not be attributed to other neurodevelopmental disorders, other mental disorders, or the “physiological effects of a substance or neurological condition” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Tic Disorders
Tics are defined as “a sudden, rapid, recurrent, nonrhythmic motor movement or vocalization” (Diagnostic and Statistical Manual of Mental Disorders, 2013). The DSM-5 (2013) includes three types of Tic Disorders: Tourette’s Disorder, Persistent (Chronic) Motor or Vocal Tic Disorder, and Provisional Tic Disorder. All three disorders have two common criteria: their onset began prior to the individual turning eighteen years old, and the disturbances are not “attributable to the physiological effects of a substance or another medical condition” (Diagnostic and Statistical Manual of Mental Disorders, 2013).
Criteria for Diagnosis
An individual is diagnosed with Tourette’s Disorder when they have multiple motor tics and one or more vocal tics. Diagnosis does not require the individual to demonstrate vocal and motor tics simultaneously, nor does it require a minimum frequency.
Persistent (Chronic) Motor or Vocal Tic Disorder is diagnosed when the individual has either motor or vocal tics, but not both. Diagnosis for both Persistent (Chronic) Motor or Vocal Tic Disorder and Tourette’s Disorder require that the tics are present and persistent for at least one year from the beginning of the first tic.
Provisional Tic Disorder is diagnosed when an individual has “single or multiple motor and/or vocal tics” that have been present for less that one year (Diagnostic and Statistical Manual of Mental Disorders, 2013).
This concludes the first class of Mental Health Diagnoses! We hope you are more knowledgeable about Neurodevelopmental Disorders, that you feel inspired to share what you have learned with others, and that you will help us stop the stigma and start a conversation about mental illness and mental health!
Up Next!
Introduction to Schizophrenia Spectrum and Other Psychotic Disorders!
References
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA, American Psychiatric Association, 2013. Web. [access date: 6 January 2018]. dsm.psychiatryonline.org